EFFECTIVE January 1, 2026
THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE READ IT CAREFULLY.
With Questions or Complaints About Your Privacy, Please Contact:
Compliance Coordinator, Casco Bay EyeCare, LLC
P.O. Box 7487, Portland, Maine 04112
Tel. 207-885-8686
SUMMARY OF YOUR RIGHTS OVER OUR USE & SHARING OF PROTECTED HEALTH INFORMATION:
- You Can Request Restrictions on Our Use or Sharing
- You Have a Right to Confidential Communications with Us
- You Can Inspect and Copy Your Medical Records
- You Can Correct or Clarify Your Medical Records
- You Have a Right to an Accounting of Our Disclosures of Protected Health Information
- You Have a Right to a Printed Copy of This Notice
- You Can Designate a Personal Representative to Act for You
- You Can Choose to Let Us Share Your Information with Family or Others Involved in Your Care
- You Can Choose to Let Us Share Your Information in Connection with Disaster Relief Situations
- You Can Choose to Allow Us to Share Your Information for Marketing or to Sell Your Information
- You Can Opt Out of Fundraising Communications
- You Have a Right to Notification of a Breach of Your Privacy
- You Can File a Complaint if You Believe We Have Violated Your Privacy Rights
SUMMARY OF WAYS WE MAY USE & SHARE YOUR PROTECTED HEALTH INFORMATION:
- For Your Treatment
- For Family Members or Others Involved in Your Care
- To Get Paid for Treating You
- To Operate Our Organization for Public Health Purposes
- To Protect Against Abuse, Neglect or Domestic Violence for Health Oversight Activities
- To Respond to Judicial or Administrative Proceedings for Law Enforcement Purposes
- To Assist Funeral Directors or Medical Examiners for Organ Donation Requests
- For Approved Medical Research
- To Prevent Threats to Health or Safety for Special Governmental Purposes for Workers’ Compensation
CASCO BAY EYECARE, LLC’S DUTIES REGARDING YOUR PROTECTED HEALTH INFORMATION:
“Protected health information” includes information regarding your past, present or future physical or mental health or condition, the health care and services provided to you, and past, present or future payment for your health care. Casco Bay EyeCare, LLC is required by law to maintain the privacy of your protected health information and to provide you with this Notice of Privacy Practices. In the event of a breach of your privacy, we are obligated to inform you promptly of the nature of the breach. We are also required to abide by the privacy practices which are currently in effect and outlined in this notice or in any amendment to this notice.
Casco Bay EyeCare, LLC reserves the right to amend or modify its privacy practices. These changes may be required by changes in federal and state laws. If we change our Notice of Privacy Practices, we will post the new Notice in our offices, have copies available in our offices and post it on our website. Any revised privacy practices will be applied to all protected health information that we maintain.
YOUR RIGHTS OVER OUR USE & SHARING OF YOUR PROTECTED HEALTH INFORMATION:
Right to Request Restrictions. You have the right to request restrictions on our use and sharing of your protected health information for purposes of treatment, payment or our organizational operations. For example, you may request that we not share your protected health information with a family member involved in your care. Or, if you pay for treatment entirely out of your own pocket, you may request that we not share information about that treatment with your health plan. Your request to restrict the use and sharing of your health information should be in writing and should be sent to our Compliance Coordinator. The request must state (i) what health information you do not want used or shared, (ii) whether you want to limit our use, limit our sharing, or both, and (iii) the names of persons or entities with whom you do not want us to share. We are not required to agree with your request. We will not agree if in our professional judgment such restrictions would affect your care. If we do agree to restrict our sharing, we may later terminate our agreement to such restrictions. Such termination will be effective only for protected health information created or received after the termination.
Right to Confidential Communications. You have the right to receive confidential communications concerning your medical condition and treatment. For example, you have the right to request that we communicate your protected health information to you at an alternate address, at an alternate phone number or by alternate means. Your request should be in writing and should be sent to our Compliance Coordinator. Your protected health information will be used by our staff to call, text and/or send you appointment reminders. Appointment reminders may take the form of messages left on an answering machine, text message, letters or post cards, but we will comply with your request to use an alternate address, phone number or means of communication.
Right to Inspect and Copy. You have the right to inspect and copy your protected health information in either paper or electronic form. If you would like to inspect or copy your protected health information, you should request an authorization form from the supervisor of our office at which you regularly have appointments or the Compliance Coordinator. We will provide access or copies within 30 days of receiving your request or explain why we need up to another 30 days. You will be charged for our reasonable costs of copying and mailing. We may deny your request in certain circumstances. For example, we may deny your request if we conclude that access to your health information will endanger your life or physical safety. If we deny your request, you may request, in a written document sent to the Compliance Coordinator, that the denial be reviewed.
Right to Correct or Clarify. You have the right to request an amendment to or submit corrections to your protected health information. The information you desire to submit should be in writing and should be sent to the Compliance Coordinator. The information you submit will be retained with our records of your treatment. If we add a statement to your treatment record in response to your submission, we will provide you with a copy of the statement.
Right to Accounting of Disclosures. You have the right to an accounting of with whom we have shared your protected health information, when and why. Your request for an accounting should be in writing and should be sent to our Compliance Coordinator. The request should state the period for which you are requesting the accounting but cannot exceed six (6) years. We will not charge you. But if you ask for another accounting within a year, we may charge you the reasonable cost of preparing the additional accounting. The “will include the date of each disclosure, the name and, if known, address of the person or entity receiving the disclosure, a brief description of the information shared and a brief statement of the purpose of sharing. We do not provide an accounting of the following disclosures: (i) disclosures for treatment, payment or health care operations, (ii) disclosures made to you, disclosures made to persons involved in your care, (iv) disclosures authorized by you, and (v) disclosures for national security or intelligence purposes, (vi) disclosures to correctional institutions or law enforcement officials.
Right to Receive a Printed Copy of this Notice. You have the right to receive a printed copy of this notice.
Right to Have Us Share Your Information with Those Involved in Your Care. You can authorize us to share protected health information with family members, close friends, or other persons involved in your care or payment for your care, to the extent relevant to their involvement with your care or payment for that care. If you are present, your protected health information will be disclosed if: (i) we obtain your agreement, (ii) we provide you with an opportunity to object and you do not object, or (iii) we reasonably assume you do not object. If you are not present, are incapacitated or it is an emergency, we may share protected information with family or other persons involved in your care to the extent that, in our professional judgment, we believe it to be in your best interest.
Right to Designate Personal Representatives. You have a right to designate someone to act on your behalf regarding your protected health information. In some cases, a court may have empowered someone to act on behalf of another individual in exercising medical decisions and privacy rights. Persons designated to act for others are called “personal representatives” and their scope of authority varies. For example, a legal guardian may have broad authority while a person designated by an individual’s limited health care power of attorney may have authority only regarding types of specific treatment or specific circumstances. Laws may also limit authority of personal representatives in certain situations.
Before we act on the direction of a personal representative, we will take reasonable steps to make sure the person has authority to act for you. For example, we will require a copy of a signed health care power appointing a personal representative, or a copy of any court order appointing a guardian, or evidence of lawful authority before we take steps involving use or sharing of protected health care information of an adult or emancipated minor.
The following table identifies who we will recognize as a personal representative for types of patients:
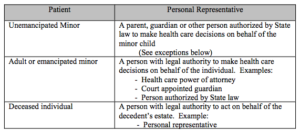
Regardless of whether a parent is the personal representative of a minor child, under certain circumstances we are prohibited from sharing the child’s protected health information with the parent. We cannot share a minor child’s protected health information with a parent under the following circumstances:
- When law does not require the consent of a parent or other person before a minor can obtain a particular health service, and the minor consents to the health service.
- When a court determines or other law authorizes someone other than a parent to make treatment decisions for a minor.
- When a parent agrees to a confidential relationship between the minor and our physician.
Under certain circumstances we may choose not to recognize a person as the personal representative of our patient. For example, if we believe that a minor child or incompetent adult patient has been or may be subjected to domestic violence, abuse or neglect by a personal representative, or that treating a person as the minor child’s or incompetent adult’s personal representative could endanger the patient, we may choose not to treat the person as the personal representative if, in our professional judgment, doing so would not be in the best interest of our patient.
Right to Share Information in Disasters. You can choose to authorize us to share protected health information in disaster relief situations. In some circumstances, when we do not have your permission, we may share this information when, in our professional judgment, doing so would be in your best interest.
Rights Concerning Marketing or Sale of Information. Our practice is not to use your protected health information for paid marketing or fundraising on behalf of others, nor will we sell your protected health information to others for any similar purpose. Even if we changed our practice to allow paid marketing for others or sale of protected health information, you would have the right to make us get your written authorization before doing so and we would have to disclose any remuneration we received.
Rights Concerning HIV Status. To the extent your protected health information in our possession includes HIV status or HIV test results, Maine law prohibits our sharing that information without your specific written authorization, subject to certain exceptions involving public safety or response to court orders.
Rights Concerning Substance Use Disorder Treatment Records. Federal law provides additional confidentiality protections for certain substance use disorder treatment records that are created by federally assisted programs. To the extent we receive, maintain, or transmit such records, we will comply with applicable federal confidentiality requirements, including 42 CFR Part 2. In some circumstances, your written authorization may be required before we may use or disclose this information, except as otherwise permitted or required by law.
Other Rights. You have other rights regarding protected health information that do not typically apply in the context of our practice.
– Hospital Directory. Because we do not maintain a directory of our patients’ status and location as a hospital might for its patients, your right to choose to have us share protected health information on a hospital directory through your written authorization is not relevant.
– Psychotherapy Notes. Because we do not maintain psychotherapy notes on our patients as a mental health provider might, your right to choose to have us share such protected health information through your written authorization is generally not relevant. If our medical records do contain psychotherapy notes forwarded to us by others, we would not share those records without your written authorization.
– Fundraising Opt-Out. Because we do not solicit our patients for fundraising, your right to opt-out of receiving fundraising communications from us is not applicable.
Right to Notice of Breach of Privacy. We will notify in writing you whenever we discover that your protected health information has been improperly used or shared, or we reasonably believe there may have been a breach of your privacy. We will notify promptly, no later than 60 days after discovery of the breach. The notice will describe in plain language what happened, when it happened, when we discovered the breach, and what type of protected health information was involved. We will tell you what steps you should take to protect yourself from potential harm from the breach and describe what we are doing to investigate the breach, to mitigate harm to you, and to protect against any further breach. We will also tell you whom to contact to ask questions or learn further details.
Right to File a Complaint. If you would like to submit a comment or complaint about our privacy practices, or obtain additional information about our privacy practices, you can do so by sending a letter outlining your concerns to the person listed below. You will not be penalized or otherwise retaliated against for filing a complaint.
Compliance Coordinator
Casco Bay EyeCare, LLC
P.O. Box 7487
Portland, Maine 04112
Tel: 207-885-8686
You may also send a complaint to the Secretary of Health and Human Services if you feel that your privacy rights have been violated. The Secretary of the Department of Health and Human Services has delegated to the Office for Civil Rights (OCR) the authority to receive and investigate complaints. Their contact information is as follows:
Region I, Office for Civil Rights
U.S. Department of Health and Human Services
Government Center, J.F. Kennedy Federal Building
Room 1875
Boston, Massachusetts 02203
Tel: 617-565-1340
Fax: 1-617-565-3809
TDD: 1-617-565-1343
WAYS IN WHICH WE MAY USE & SHARE YOUR PROTECTED HEALTH INFORMATION:
For Your Treatment. Our physicians and staff members may use your protected health information or may share it with other health care professionals for purposes of evaluating your health, diagnosing medical conditions, and providing treatment. Your protected health information may be used to send you information on the treatment and management of your medical condition that you may find to be of interest. We may also send you information describing other health-related goods and services that we believe may benefit you. However, without your written permission, we will not use your protected health information for marketing for which we are paid by others, nor will we sell your protected health information to anyone else.
For Family Members or Other Persons Involved in Your Care. We may share your protected health information with your family member, other relative, close friend or other person you identify. Disclosures will be limited to your protected health information that is relevant to such family member or other person’s involvement in your care or payment for your care. If you are present, your protected health information will be shared if: (i) we obtain your agreement, (ii) we provide you with an opportunity to object and you do not object, or (iii) we reasonably assume you do not object. If you are not present or you do not have an opportunity to object or agree because you are incapacitated, or it is an emergency, we may share protected information to the extent that, in our professional judgment, we believe it to be in your best interest.
For Payment. We may use your protected health information to seek payment from your health plan or other sources of coverage such as an automobile insurer, or credit card companies that you may use to pay for services. For example, your health plan may request and receive information on dates of service, the services provided, and the medical condition being treated. Where you have paid for treatment yourself and have requested that we not share information about those services with your health plan, we will not share protected health information regarding that service with your health plan, unless required by law.
For Organizational Operations. We may use your protected health information as necessary to support the day- to- day activities and management of Casco Bay EyeCare, LLC. For example, information on the services our patients receive may be used to support budgeting and financial reporting and activities to evaluate and promote quality to ensure that our practice is meeting state and federal laws regarding your protected health care information. Protected health information is also used by to coordinate staffing with patient treatment needs, and schedule appointments and provide appointment reminders.
For Public Health Reporting. We may share your protected health information with public health agencies as required by law. For example, our practice is required to report certain communicable diseases to State of Maine Department of Health. We may also be required to report the Federal Food & Drug Administration on matters affecting the quality or safety of regulated drugs or products.
To Prevent Abuse, Neglect or Domestic Violence. Our physicians and staff may be required to report to social service agencies or law enforcement agencies those cases in which we reasonably suspect a minor or incapacitated person may be a victim of abuse or neglect. Additionally, we may be required to report cases of abuse, neglect or domestic violence when, in our professional judgment, we believe reporting necessary to prevent serious harm. We will notify you or your personal representative of our reporting suspected abuse, neglect or domestic violence, unless we believe, in our professional judgment, that notifying you would risk serious harm to you or that it would not be in your best interest to report to your personal representative because we reasonably believe the personal representative may be responsible for the suspected wrongful acts.
For Health Oversight Activities. We may share your protected health information with a health oversight agency for oversight activities authorized by law. These activities include audits of health care providers, investigations of civil, criminal or administrative violations, inspections to ensure proper delivery of healthcare, professional licensure or disciplinary actions, and other activities for oversight of our healthcare system or government healthcare benefits.
For Judicial and Administrative Proceedings. We may disclose your protected health information to comply with a court or administrative order, to the extent that order expressly authorizes sharing protected health information. In addition, your protected health information may be disclosed to comply with a subpoena, discovery request or other lawful process that is not accompanied by a court order if (i) we receive satisfactory assurances that reasonable efforts have been made to ensure that you have been given notice of the request, or (ii) we receive satisfactory evidence that reasonable efforts have been made to secure a qualified protective order.
For Law Enforcement Purposes. We may share your protected health information with law enforcement officials for law enforcement purposes, as required by law. For example, we will share your protected health information on the request of a law enforcement official if you are or are suspected to be a victim of a crime, we are unable to obtain your authorization in the circumstances, and, in our professional judgment, we believe that sharing the information would be in your best interests.
For Funeral Director or Medical Examiner Uses. We may share your protected health information with funeral directors as necessary for them to provide services, or medical examiners or coroners as necessary for them to perform their duties.
For Organ Donation Requests. If you are an organ donor, we may share your protected health information with organizations that engage in the procurement, banking or transportation of organs, eyes or tissues for transplantation or donation.
For Medical Research. We may share your protected health information for use in for authorized medical research. We will not share your protected health information until we have documentation of appropriate privacy board review of any research project, or we have representations by the researcher of need for access to protected health information (not to be removed from our premises) to prepare a medical research proposal.
To Prevent Threats to Health or Safety. We may share your protected health information if, in good faith, we believe that it is necessary to prevent or limit a serious and imminent threat to the health and safety of a person or the public. For instance, we may alert a person who is the subject of a threat of physical harm, or we may alert a law enforcement officer to help identify or apprehend a violent criminal or an escaped prisoner.
For Specialized Government Functions. We may share your protected health information for certain specialized government functions, as provided by law. For instance, if you are a member of the armed forces, your protected health information may be shared with military authorities as required by them. If you are an inmate, we may share your protected health information with the correctional facility for the safety of you, other inmates and correctional employees. We may share your protected health information with authorized federal officers for purposes of protecting the President or other governmental officers, or for the conduct of intelligence, counterintelligence or other national security purposes.
Workers’ Compensation Purposes. We may share your protected health information as necessary to comply with workers’ compensation laws or similar programs that provide benefits for work-related injuries.
Other authorized uses and disclosures. You may authorize us to use and share your protected health information for purposes other than those listed above. Your authorization must be in writing and must comply with applicable law. If you change your mind after authorizing the use or sharing of your protected health information, you may submit a written revocation of the authorization. However, your decision to revoke the authorization will not affect or undo any use or disclosure of protected health information that occurred before you notified us of your decision.